Skip to content
Skip to content
The anxiety is almost always worse than the procedure.
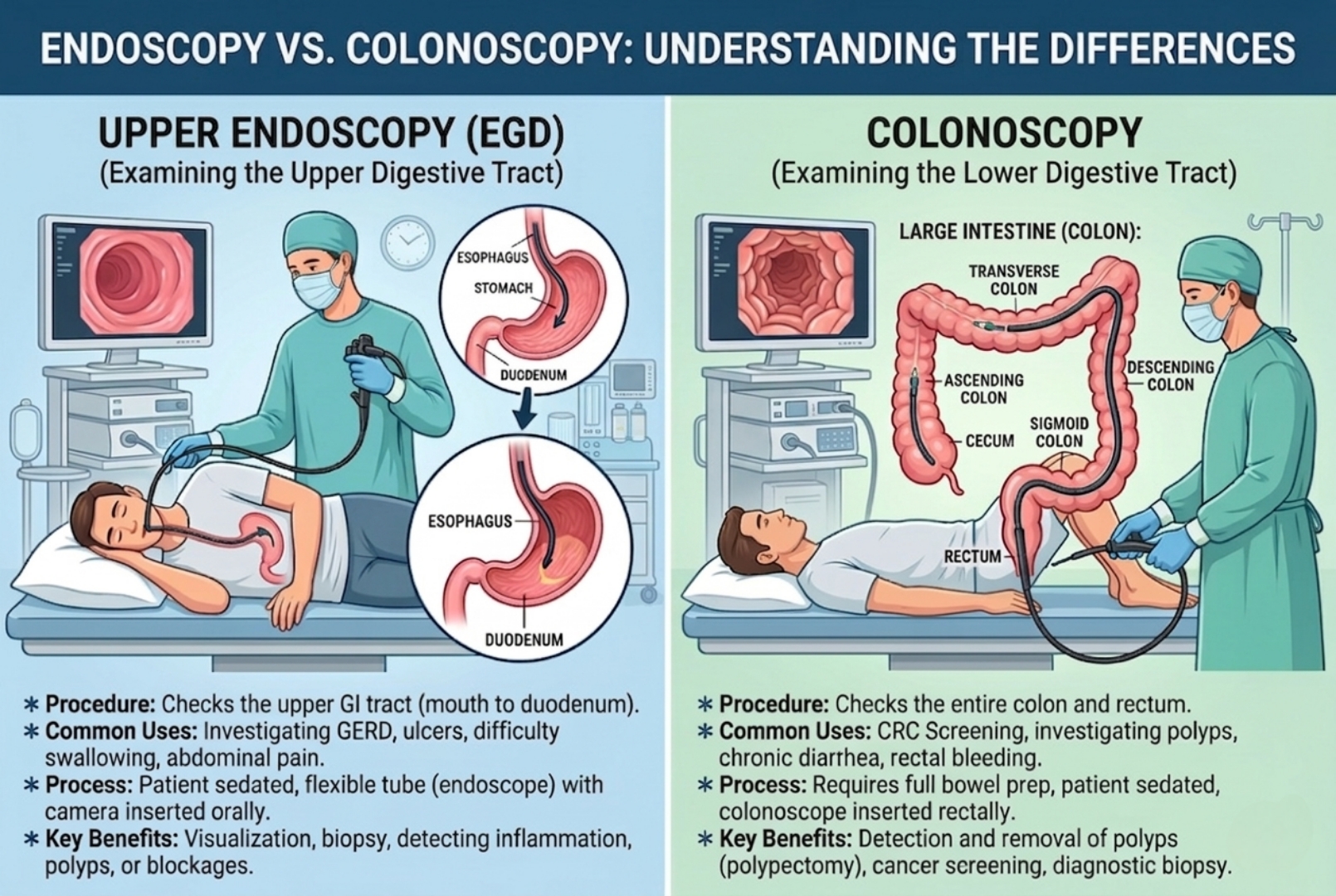
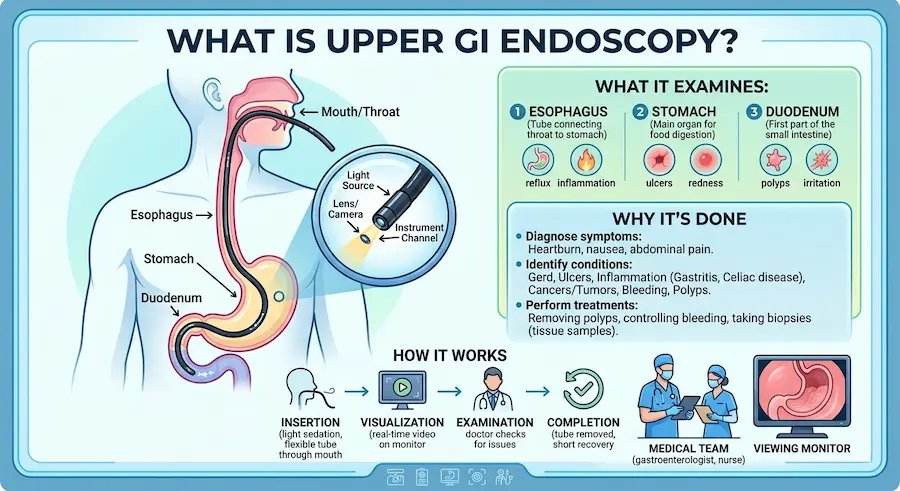
An upper GI endoscopy takes 5–15 minutes, uses a numbing spray or light sedation, and gives your doctor a direct look at what blood tests can’t show. Here’s exactly what to expect.
Are you avoiding an endoscopy because you’re scared?
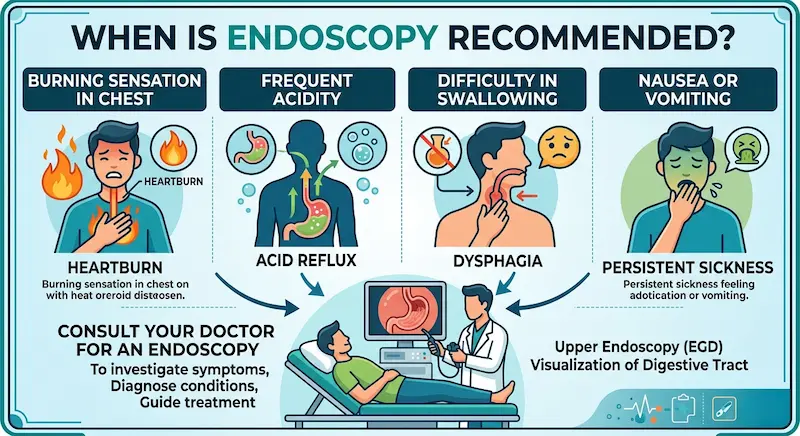
When a doctor recommends an upper GI endoscopy, most people picture pain, surgery, or a complicated ordeal — one of the biggest reasons patients delay diagnosis, even with symptoms like persistent acidity, difficulty swallowing, stomach pain, or unexplained weight loss. In reality, most patients are surprised by how quick and manageable it is.
A thin, flexible camera — four stops, one clear picture.
Mouth & throat
The scope enters gently after a throat-numbing spray, so the initial pressure most people worry about barely registers.
Where sedation takes effectEsophagus (food pipe)
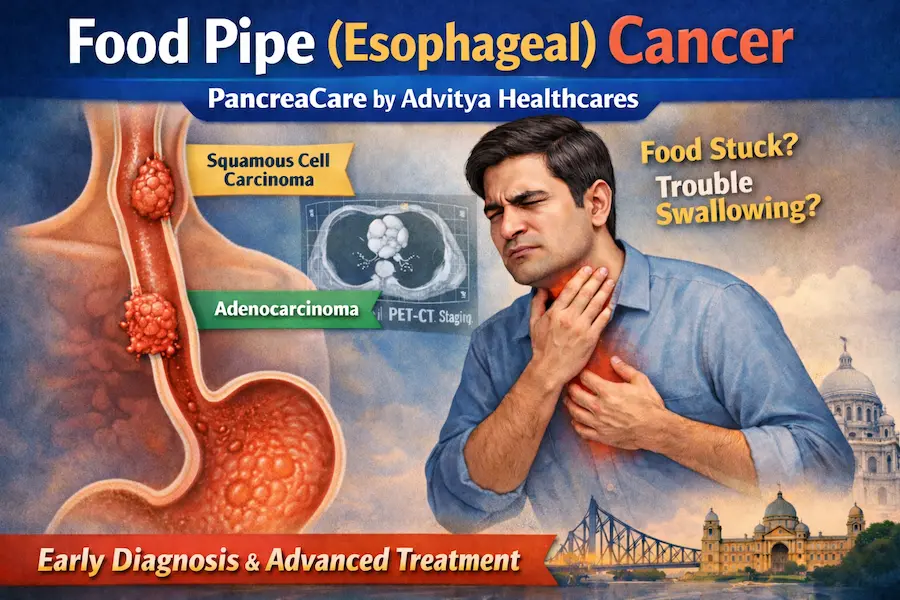
The camera checks the lining for narrowing, inflammation, or Barrett’s esophagus — changes that rarely show up on a scan.
Detects: reflux damage, stricturesStomach
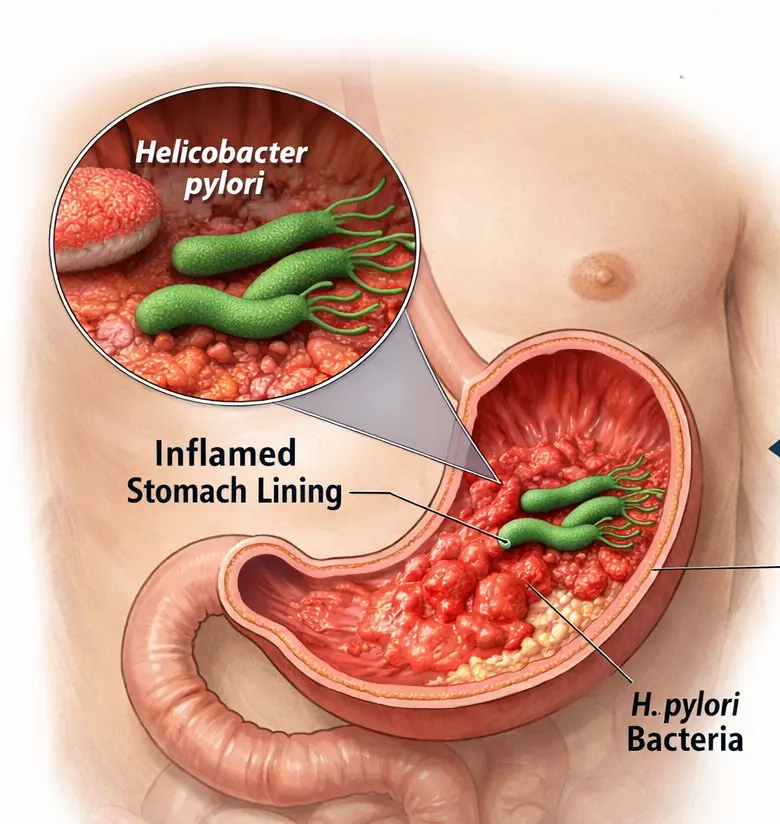
A full view of the stomach lining reveals gastritis, ulcers, polyps, or infections like H. pylori — and lets your doctor take a painless tissue sample if needed.
Detects: ulcers, gastritis, H. pyloriDuodenum
The first part of the small intestine is examined for early signs of inflammation or malabsorption issues before symptoms escalate.
Detects: early-stage abnormalitiesMost patients receive a throat-numbing spray and, in many cases, mild sedation to stay relaxed throughout. Any discomfort as the scope passes is brief. Many patients later say the anxiety beforehand was worse than the procedure itself.
Faster than most people imagine.
The gap between noticing a symptom and doing something about it.
The same starting point leads to very different outcomes, depending on what happens next.
Symptoms get self-medicated, not diagnosed
- Acidity managed with over-the-counter tablets
- Underlying ulcers or gastritis stay hidden
- Simple issues have room to progress
A 15-minute look, then a clear plan
- Exact cause identified, not guessed at
- Biopsy taken on the spot if needed, painlessly
- Treatment starts while it’s still simple
One look can catch what blood work and scans miss.
Gastritis
Inflammation of the stomach lining, often silent until it’s advanced.
Peptic ulcers
Sores that can bleed or worsen if left undiagnosed.
Barrett’s esophagus
A precancerous change linked to long-term acid reflux.
Esophageal narrowing
A structural cause of persistent swallowing difficulty.
H. pylori infection
A common, treatable cause of chronic stomach pain.
Polyps & early cancers
Caught earliest, these are the easiest to treat successfully.
Tap a card to flip it.
Most of the fear around endoscopy comes from outdated ideas, not the actual procedure.
It’s extremely painful.
Tap to see the fact →Most patients feel little to no pain. Numbing spray and sedation make it comfortable.
It’s a surgery.
Tap to see the fact →It’s a non-surgical diagnostic procedure — no cuts, no stitches.
It takes hours.
Tap to see the fact →The examination itself usually takes just 5–15 minutes.
Recovery takes days.
Tap to see the fact →Most patients return to their normal routine within 24 hours.
Only older adults need one.
Tap to see the fact →Digestive disorders affect adults of any age — persistent symptoms shouldn’t be ignored.
A biopsy will hurt.
Tap to see the fact →Tissue sampling is painless — the stomach lining has no pain-sensitive nerve endings.
How to prepare
A few simple steps make for a smoother procedure and more accurate results.
- 1Fast for 6–8 hours
No food or drink in the window before your procedure.
- 2Share your medication list
Tell your doctor about all medications and allergies.
- 3Flag blood thinners or diabetes
These change how your prep is managed.
- 4Arrange a ride home
If sedation is planned, avoid driving for the rest of the day.
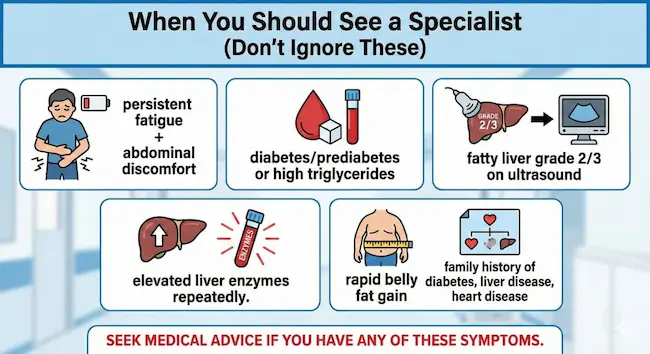
Don’t dismiss these as “just gas.”
Digestive diseases often begin with mild, easy-to-ignore symptoms. Left unchecked, ulcers, inflammation, or worse can progress. An early endoscopy catches problems while treatment is still simple.
Talk to a GI specialist if you notice:
- Persistent acidity despite medication
- Difficulty swallowing
- Frequent vomiting
- Blood in vomit or black stools
- Unexplained weight loss
- Severe upper abdominal pain
- Long-term indigestion
- Family history of GI cancers
Better digestive health starts with one clear look.
Our GI surgery team provides comprehensive evaluation and advanced diagnostics, including upper GI endoscopy, with accurate diagnosis and compassionate, personalized care.