PancreaCare by
Advitya Healthcares
___________________________________________
National Cancer Prevention Month
Written for patients and their families — plain language, real answers.
___________________________________________
Covering: Oesophageal | Stomach | Liver | Gallbladder | Bile Duct
Pancreatic | Small Bowel | Colon | Rectal | Anal | GIST | NETs
| IMPORTANT NOTICE This blog is for general health education only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always speak with your own doctor or specialist about your personal health situation. |
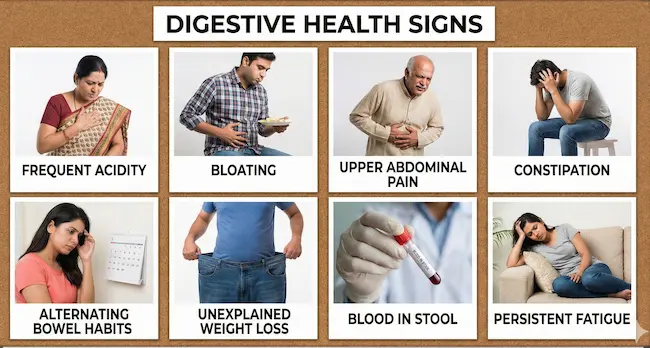
Warning Signs: When to See a Doctor
No matter which GI cancer we’re talking about, certain symptoms should always prompt a visit to your doctor without delay. They don’t automatically mean cancer — but they always deserve investigation:
| Red Flag Symptoms — Never Ignore These Unexplained weight loss or loss of appetite Difficulty swallowing or pain when swallowing Persistent indigestion, heartburn, or abdominal pain Vomiting blood, or vomit that looks like coffee grounds Black, tarry, or bloody stools New jaundice — yellowing of skin or whites of the eyes Dark urine and pale/clay-coloured stools A change in bowel habits lasting more than 3 weeks Unexplained new anaemia (low blood count) New-onset diabetes after age 50, especially with weight loss A lump or swelling in the abdomen If you have any of these — please make an appointment with your GP today. Early detection genuinely saves lives. |
| About This Guide This guide is brought to you by PancreaCare by Advitya Healthcares.This is one section from a 12-part GI cancer series, and each section follows the same structure—what it is, why it happens, how to lower your risk, how it’s diagnosed, how it’s treated (including what surgery involves), and what recovery looks like—so you can use the headings to jump to what you need, or read straight through, because knowledge is the best first step. |
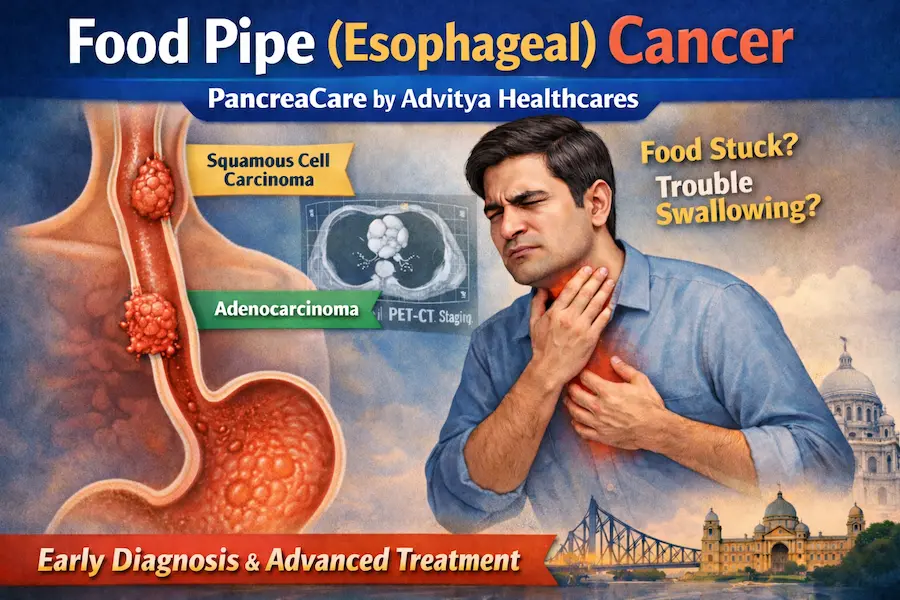
Stomach Cancer – Gastric Cancer
What Is It?

The stomach is a muscular bag that sits just below your ribcage on the left side. It mixes food with acid and digestive juices before passing it into the small bowel. Stomach cancer — also called gastric cancer — usually starts in the inner lining of the stomach.
Most stomach cancers are adenocarcinomas (starting in gland cells). Less common types include lymphoma, GIST (a tumour of the stomach wall), and carcinoid tumours. It often develops slowly over many years from inflammation or precancerous changes.
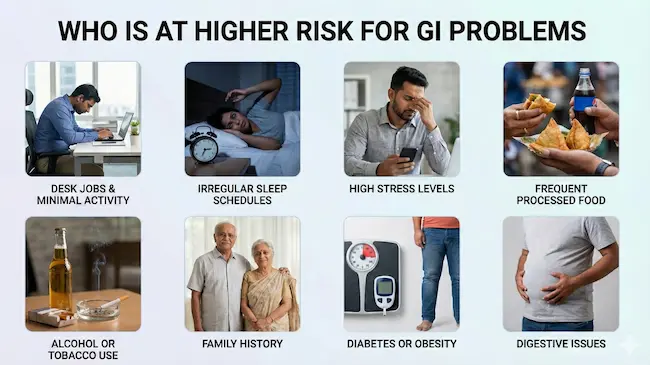
Why Does It Happen? (Causes & Risk Factors)

Stomach cancer tends to build quietly over time, driven by a mix of infection, lifestyle, and genetics:
- Smoking
- A diet high in salty, smoked, preserved, or pickled foods
- Low intake of fresh fruit and vegetables
- Chronic gastritis or precancerous stomach changes (intestinal metaplasia, dysplasia)
- Family history of stomach cancer
- Conditions like pernicious anaemia or previous stomach surgery
- H. pylori (Helicobacter pylori) bacterial infection — a very common, treatable bug that can cause long-standing inflammation
How Can I Lower My Risk?

Prevention is very much possible — especially by targeting H. pylori:
- Stop smoking
- Eat more fresh fruit and vegetables, and less salt-preserved or processed food
- Treat persistent indigestion or stomach symptoms — don’t ignore them
- If you have a strong family history, discuss surveillance options with your doctor
- Get tested for H. pylori — a simple breath or stool test can detect it, and a short course of antibiotics clears it
How Is It Diagnosed?

Early stomach cancer often has no clear symptoms, which is why acting on indigestion, unexplained weight loss, or early fullness is important:
- Upper GI endoscopy (OGD) with biopsies: the key diagnostic test
- CT scan: to stage the cancer and check for spread
- Endoscopic ultrasound (EUS): assesses the depth of invasion
- PET scan: in selected cases
- Staging laparoscopy: a keyhole look inside the abdomen before surgery to rule out hidden spread
How Is It Treated?

Treatment is tailored to the stage and the individual:
- Early-stage (confined to lining): endoscopic mucosal resection may be sufficient
- Operable cancers: surgery is the cornerstone, often with chemotherapy before and after
- HER2-positive tumours: targeted therapy (trastuzumab) added to chemotherapy
- Advanced: chemotherapy, immunotherapy, and supportive care
| The Surgery: Gastrectomy A gastrectomy removes part (partial) or all (total) of the stomach, along with nearby lymph nodes. Partial gastrectomy: removes the lower part of the stomach; the remainder is reconnected to the small bowel. Total gastrectomy: the entire stomach is removed; the oesophagus is connected directly to the small bowel. Both operations are typically done by keyhole surgery where possible. The operation takes 3-6 hours. Hospital stay is around 7-10 days. |
Aftercare & Recovery

Life after gastrectomy takes adjustment, but most people manage very well with the right guidance:
- Eat small, frequent meals — 5 to 6 times a day rather than 3 large ones
- Avoid very sweet foods to prevent ‘dumping syndrome’ (feeling dizzy or unwell after eating)
- Vitamin B12 injections every 3 months (the stomach makes a protein needed to absorb B12)
- Iron and calcium supplements as advised
- Regular follow-up scans and endoscopy
| Dumping syndrome — feeling flushed, sweaty, or unwell soon after eating — is common after stomach surgery but usually improves with dietary changes. Your dietitian will guide you through what to eat and what to avoid. |










")