
Symptoms People Miss in the
“Stone Belt”
In and around Ranchi, gallbladder stones are so common that many people learn to “live with them.” A pain episode happens, they take antacids, avoid oily food for a few days, and move on. The problem is not that gallstones are always dangerous—most people with gallstones never develop cancer—but that this habit of ignoring symptoms can delay the diagnosis of gallbladder cancer, which often stays subtle until it becomes advanced.
Across north and east India, higher gallbladder cancer burden is strongly clustered in the Indo-Gangetic / Gangetic (and broader Ganga–Brahmaputra) belt, and gallstones are an associated factor in these regions.
So this blog is a “field guide” for Ranchi patients and families:
When is it “just stones,” and when should you worry about cancer?
First truth: Gallstones are common. Gallbladder cancer is not.
Let’s reduce fear and increase precision.
- Gallstones are the most common risk factor associated with gallbladder cancer, but most people with gallstones never get cancer.
- In Indian data, gallstones are found in a large proportion of gallbladder cancer patients (often cited around 60–90%), but only a small fraction of all gallstone patients develop cancer—one review notes roughly 1–3%.
- Incidental gallbladder cancer (found unexpectedly after gallbladder removal for stones) has been reported in about 0.19%–1.6% of cholecystectomy specimens (mean ~0.36%).
- Across studies, gallstone disease has been associated with higher gallbladder-cancer risk (reported ~2–24×), and gallstones are present in a high proportion of gallbladder cancer cases (e.g., ~86% in one cited dataset).
Meaning: You don’t panic. You watch for high-risk patterns.
The danger link: Large, long-standing stones → chronic irritation
“Chronic inflammation” is the bridge
Long-term friction and inflammation of the gallbladder lining is a key pathway discussed in clinical literature for how stones can contribute to cancer risk over time.
The big stone red flag (≥ 3 cm)
This is one of the most practical, evidence-backed risk signals:
- A classic study found a strong association between stone size and gallbladder cancer; where larger stones (often considered to be more than ≥ 2 cm) were associated with a much higher relative risk than small stones.
- India’s ICMR consensus document summarises that larger stones are associated with increased risk (RR roughly ~9–10 in cited evidence) and that long duration (e.g., >20 years) also increases risk.
In simple words: If someone has a very large stone or stones for many years, it should not be treated casually—especially if symptoms are changing.
“Stones” vs “Cancer”: the symptom pattern that separates them
Many early cancer symptoms mimic gallstone disease. What matters is the pattern.
Typical gallstone pain
- Sudden pain in upper right abdomen (often after oily food)
- Comes in waves, improves with time/meds
- May recur as “attacks”
Cancer-leaning clues (often ignored in Ranchi)
Gallbladder cancer can be vague at first, but common warning symptoms include persistent right-upper abdominal pain, bloating, loss of appetite/weight loss, a palpable mass, and sometimes jaundice (often later).
Take these seriously if they persist or are new:
- Pain that becomes persistent (a constant “dragging” discomfort, not just attacks)
- Unexplained weight loss or appetite drop
- Itching + dark urine + pale stools, especially with jaundice (suggests bile blockage)
- A lump/fullness in the right upper abdomen
- Symptoms that don’t fit your “usual stone attacks” (you know your body—if it’s different, investigate)

The clinic checklist that raises suspicion
When to suspect Gall Bladder Carcinoma in a patient with Gallstone Disease?”
Clinical background that increases suspicion
- Age > 65 years
- Female sex (seen in many series)
- High-incidence regions/ethnic risk background (e.g., Asian populations)
Symptom red flags (especially if they don’t match “typical” stone attacks)
- Jaundice without acute cholecystitis (reported OR ~2.2 in one cited study)
- Weight loss > 10% (unintentional)
- Vague or persistent upper abdominal pain (not just episodic colic)
- Mismatch between symptoms and imaging findings (a “scan–symptom mismatch”)
Blood test clues (LFT pattern)
- Raised total and/or direct bilirubin
- Alkaline phosphatase (ALP) > 120 U/L (reported OR ~1.7 in one cited study)
- Unexplained elevation of liver enzymes / “abnormal LFTs” without a clear cause
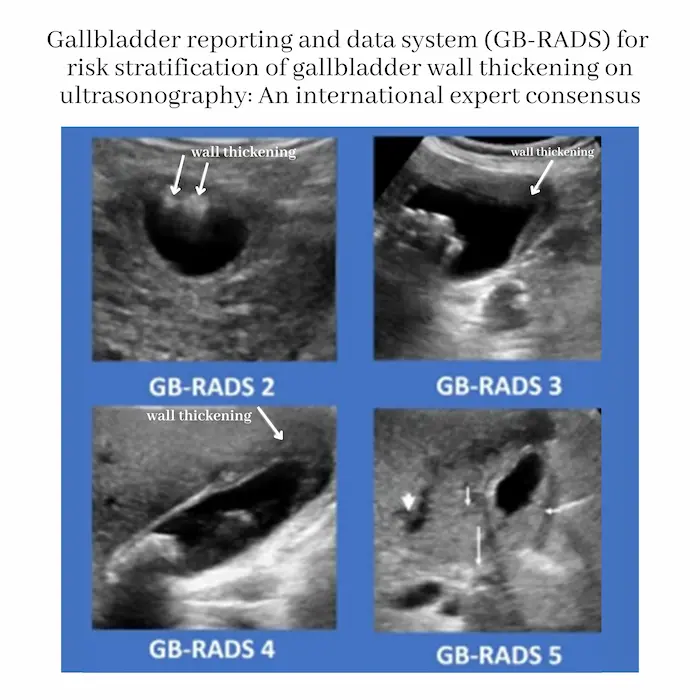
Radiology: what to look for on USG/MRI (ask for structured reporting if available)
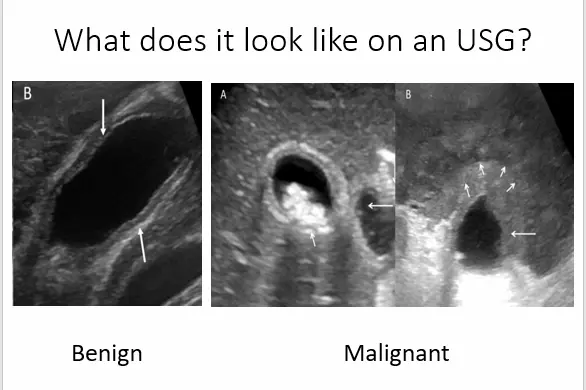
- Ultrasound (USG): focal/asymmetric wall thickening (often > 5 mm), irregularity, breach of the mucosal line, inhomogeneous echogenicity, or increased vascularity; a discrete mass is strongly suspicious.
- MRI: malignant wall thickening may appear T2-hyperintense with diffusion restriction and show earlier enhancement; mucosal breach or loss of mural layering increases concern.
- GB-RADS (expert consensus) is a structured way to report gallbladder lesions and communicate “how suspicious” the findings are.
Why multiple red flags matter: one cited analysis reported a 47.4-fold increase in risk when 4 risk factors were present together. So the goal is not to fear a single symptom, but to escalate work-up when several red flags cluster.
High-risk “Stone Belt” situations where you shouldn’t delay surgery/workup
Consider a faster HPB (liver–pancreas–bile duct) evaluation when you have gallstones plus any of these:
- Large stone
- Very long history of stones / chronic cholecystitis
- Porcelain gallbladder (calcified gallbladder wall) — risk is debated today but still treated cautiously, especially if symptomatic
- Gallbladder polyp ~≥ 7-8 mm, or those increasing in size (many guidelines recommend cholecystectomy at this size threshold)
- Recurrent symptoms + imaging that shows a mass, irregular gallbladder wall thickening, or suspicious findings
The key surgical point (your message is correct — here’s the precise version)
If cancer is suspected, a simple gallbladder removal is usually not enough.
For suspected/confirmed gallbladder cancer beyond the earliest stage, standard oncologic surgery is typically an extended (radical) cholecystectomy, not just removing the gallbladder.
Radical/extended cholecystectomy generally includes:
- Removing the gallbladder en bloc
- Removing a wedge of liver from the gallbladder bed (often ~2–3 cm margin) or a formal segment IVb/V resection
- Regional lymph node dissection (hepatoduodenal ligament/pericholedochal nodes and related stations) for staging and local control
Why this matters: gallbladder cancer spreads early through lymphatics and into the liver bed; radical surgery aims to remove microscopic spread and reduce recurrence risk.
What’s genuinely new right now
If you want “what’s new” that’s real (not hype), here are three credible shifts:
- Clearer global surgical consensus (2024): International HPB groups have been publishing consensus-style guidance to standardize definitions—what exactly counts as “radical resection,” how much liver, which lymph nodes, and terminology across early/incidental/advanced disease.
- Minimally invasive radical surgery is expanding (but center-dependent): Reviews and meta-analyses (2024–2025) suggest robotic/laparoscopic radical cholecystectomy can be feasible and safe in selected patients when done by experienced teams, while acknowledging most evidence is still retrospective and expertise-dependent.
- More “early detection” research: There’s active work on earlier detection strategies and biomarkers in high-incidence regions, reflecting how urgent this is in India’s belt areas.
Action checklist
If someone in the family has gallstones, ask these 5 quick questions:
- Has the pain changed from “attacks” to a persistent daily discomfort?
- Any weight loss / appetite loss without trying?
- Any itching, dark urine, pale stools, or jaundice?
- Are any large stones found on ultrasound/CT?
- Did imaging mention a mass, irregular thickening, or suspicious polyp (around ≥1 cm)?
If 2 or more are “yes,” don’t treat it as routine acidity—get an HPB evaluation and proper imaging.
Leave a Reply
You must be logged in to post a comment.